Children’s Abrasions in Recreational Beach Areas and a Review of Possible Wound Infections


Abstract
:1. Introduction
1.1. Behavior
1.2. Pathogens
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion and Recommendations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
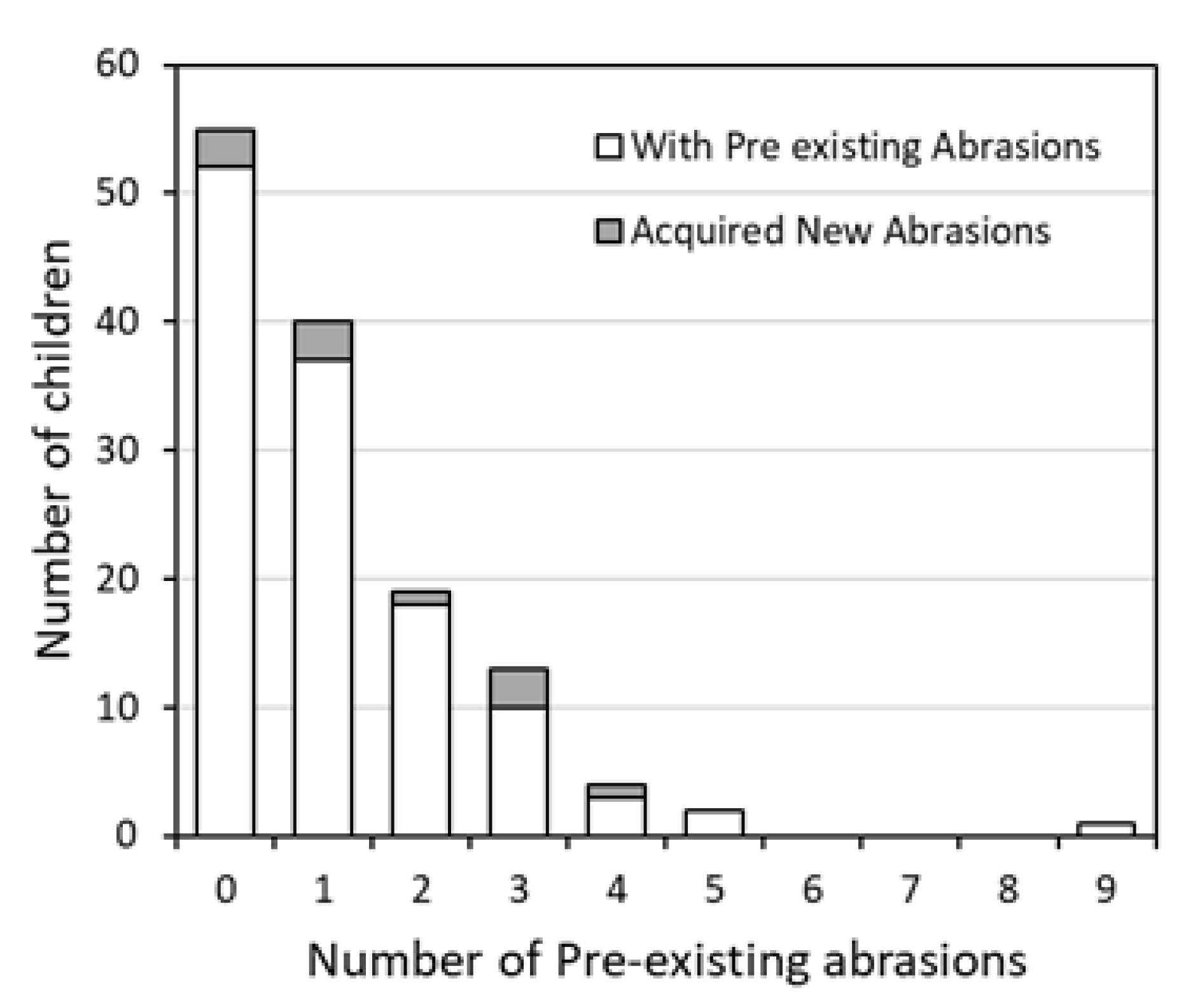
| Number of Pre-Existing Abrasions Before 1 Hour of Play | Percentage of Children Who Acquired New Abrasions During 1 Hour of Play (%) | Ratio of Children Who Acquired New Abrasions During 1 Hour of Play | Confidence Interval |
|---|---|---|---|
| 0 | 5.8% | 3/52 | 0.012 to 0.162 |
| 1 | 5.7% | 3/37 | 0.007 to 0.182 |
| 2 | 5.3% | 1/18 | 0.001 to 0.273 |
| 3 | 30.0% | 3/10 | 0.067 to 0.653 |
| 4 | 33.3% | 1/3 | 0.008 to 0.906 |
| 5 | 0 | 0/2 | N/A a |
| 6 | 0 | 0/0 | N/A |
| 7 | 0 | 0/0 | N/A |
| 8 | 0 | 0/0 | N/A |
| 9 | 0 | 0/1 | N/A |
References
- Griffin, J. Another Case of Flesh-Eating Bacteria Sends Tarpon Springs Fisherman to the Hospital. Tampa Bay Times. Available online: https://www.tampabay.com/health/another-case-of-flesh-eating-bacteria-sends-tarpon-springs-fisherman-to-the-hospital-20190731/ (accessed on 22 September 2019).
- Ocasio, B.P. Man Recovers from Flesh-Eating Infection after Spring Break Swim in a Florida River. Miami Herald. Available online: https://www.miamiherald.com/living/health-fitness/article233522322.html (accessed on 22 September 2019).
- Park, K.H.; Hwang, J.H.; Jung, S.I.; Shin, J.H.; Jung, Y.S. Marine bacteria as a leading cause of necrotizing fasciitis in coastal areas of South Korea. Am. J. Trop. Med. Hyg. 2009, 80, 646–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florida Department of Health. Vibrio Infections. Available online: http://www.floridahealth.gov/diseases-and-conditions/vibrio-infections/vibrio-vulnificus/index.html (accessed on 9 October 2019).
- Florida Department of Health. What You Need to Know about Necrotising Fasciitis; Commonly Called “Flesh-Eating Bacteria.” Florida Department of Health in Hillsborough County. Available online: http://hillsborough.floridahealth.gov/newsroom/2019/07/NECROTIZING_FASCIITIS.html (accessed on 23 August 2019).
- Ferguson, A.; Del Donno, C.; Obeng-Gyasi, E.; Mena, K.; Kaur Altomare, T.; Guerrero, R.; Gidley, M.; Montas, L.; Solo-Gabriele, H.M. Children exposure behavior patterns and risk perception with recreational beach use. Int. J. Env. Res. Public Health 2019, 16, 2783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United States Lifesaving Association (USLA). USLA—Statistics. Available online: http://arc.usla.org/Statistics/public.asp (accessed on 22 August 2019).
- Brinks, M.V.; Dwight, R.H.; Osgood, N.D.; Sharavanakumar, G.; Turbow, D.J.; El-Gohary, M.; Caplan, J.S.; Semenza, J.C. Health risk of bathing in Southern California coastal waters. Arch. Environ. Occup. Health 2008, 63, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Schets, F.M.; Schijven, J.F.; Husman, A.M.D.R. Exposure assessment for swimmers in bathing waters and swimming pools. Water Res. 2011, 45, 2392–2400. [Google Scholar] [CrossRef]
- Kueh, C.; Kutarski, P.; Brunton, M. Contaminated marine wounds-the risk of acquiring acute bacterial infection from marine recreational beaches. J. Appl. Bacteriol. 1992, 73, 412–420. [Google Scholar] [CrossRef]
- Holtcamp, W. In the same boat? Health risks of water recreation are not limited to full-contact activities. Environ. Health Perspect. 2012, 120. [Google Scholar] [CrossRef]
- Young, S.J.; Barnett, P.L.J.; Oakley, E.A. 10. Bruising, abrasions and lacerations: Minor injuries in children I. Med. J. Aust. 2005, 182, 588–592. [Google Scholar] [CrossRef]
- Lipp, E.K.; Kurz, R.; Vincent, R.; Rodriguez-Palacios, C.; Farrah, S.R.; Rose, J.B. The effects of seasonal variability and weather on microbial fecal pollution and enteric pathogens in a subtropical estuary. Estuaries 2001, 24, 266. [Google Scholar] [CrossRef]
- Lipp, E.K.; Rodriguez-Palacios, C.; Rose, J.B. Occurrence and distribution of the human pathogen Vibrio vulnificus in a subtropical Gulf of Mexico estuary. Ecol. Etiol. New. Emerg. Mar. Dis. 2001, 24, 165–173. [Google Scholar] [CrossRef]
- Lin, M.; Payne, D.A.; Schwarz, J.R. Intraspecific diversity of Vibrio vulnificus in Galveston Bay water and oysters as determined by randomly amplified polymorphic DNA PCR. Appl. Environ. Microbiol. 2003, 69, 3170–3175. [Google Scholar] [CrossRef] [Green Version]
- Mathai, P.P.; Dunn, H.M.; Magnone, P.; Zhang, Q.; Ishii, S.; Chun, C.L.; Sadowsky, M.J. Association between submerged aquatic vegetation and elevated levels of Escherichia coli and potential bacterial pathogens in freshwater lakes. Sci. Total Environ. 2019, 657, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Bravo, A.; Kilgore, P.B.; Andersson, J.A.; Blears, E.; Figueras, M.J.; Hasan, N.A.; Colwell, R.R.; Sha, J.; Chopra, A.K. T6SS and ExoA of flesh-eating Aeromonas hydrophila in peritonitis and necrotizing fasciitis during mono- and polymicrobial infections. Proc. Natl. Acad. Sci. USA 2019, 116, 24084–24092. [Google Scholar] [CrossRef] [PubMed]
- Plano, L.R.W.; Shibata, T.; Garza, A.C.; Kish, J.; Fleisher, J.; Sinigalliano, C.D.; Gidley, M.L.; Withum, K.; Elmir, S.M.; Hower, S.; et al. Human-associated methicillin-resistant Staphylococcus aureus from a subtropical recreational marine beach. Microb Ecol. 2013, 65, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Baker-Austin, C.; Oliver, J.D. Vibrio vulnificus: New insights into a deadly opportunistic pathogen. Environ. Microbiol. 2017, 20, 423–430. [Google Scholar] [CrossRef] [Green Version]
- Shaw, K.S.; Sapkota, A.R.; Jacobs, J.M.; He, X.; Crump, B.C. Recreational swimmers exposure to Vibrio vulnificus and Vibrio parahaemolyticus in the Chesapeake Bay, Maryland, USA. Environ. Int. 2015, 74, 99–105. [Google Scholar] [CrossRef]
- Kelly, M.T. Effect of temperature and salinity on Vibrio (Beneckea) vulnificus occurrence in a gulf coast environment. Appl. Environ. Microbiol. 1982, 44, 820–824. [Google Scholar] [CrossRef] [Green Version]
- Nigro, O.D.; Hou, A.; Vithanage, G.; Fujioka, R.S.; Steward, G.F. Temporal and spatial variability in culturable pathogenic Vibrio spp. in Lake Pontchartrain, Louisiana, following Hurricanes Katrina and Rita. Appl. Environ. Microbiol. 2011, 77, 5384–5393. [Google Scholar] [CrossRef] [Green Version]
- Oliver, J.D. Wound infections caused by Vibrio vulnificus and other marine bacteria. Epidemiol. Infect. 2005, 133, 383–391. [Google Scholar] [CrossRef]
- Wetz, J.; Blackwood, A.; Fries, J.; Williams, Z.; Noble, R. Trends in total Vibrio spp. and Vibrio vulnificus concentrations in the eutrophic Neuse River Estuary, North Carolina, during storm events. Aquat. Microb. Ecol. 2008, 53, 141–149. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). Preliminary Incidence and Trends of Infections with Pathogens Transmitted Commonly through Food—Foodborne Diseases Active Surveillance Network, 10 U.S. Sites, 2006–2017. Morb. Mortal. Wkly. Rep. 2018, 67, 324–328. [CrossRef]
- Horseman, M.A.; Surani, S. A comprehensive review of Vibrio vulnificus: An important cause of severe sepsis and skin and soft-tissue infection. Int. J. Infect. Dis. 2011, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, M.K.; Oliver, J.D. Vibrio vulnificus: Disease and pathogenesis. Infect. Immun. 2009, 77, 1723–1733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rippey, S.R. Infectious diseases associated with molluscan shellfish consumption. Clin. Microbiol. Rev. 1994, 7, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Bross, M.H.; Soch, K.; Morales, R.; Mitchell, R.B. Vibrio vulnificus Infection: Diagnosis and treatment. Am. Fam. Physician 2007, 74, 539–544. [Google Scholar]
- Gulf Research Initiative (GRI). Available online: https://data.gulfresearchinitiative.org (accessed on 19 April 2020). [CrossRef]
- Pezzullo, J.C. Exact Binomial and Poisson Confidence Interval. Stat Pages. 2019. Available online: http://statpages.info/confint.html (accessed on 9 October 2019).
- Select Statistical Services (SSS). Odds Ratio—Confidence Interval. Available online: https://select-statistics.co.uk/calculators/confidence-interval-calculator-odds-ratio/ (accessed on 9 October 2019).
- Riviera, S.; Lugo, T.; Hazen, T.C. Autecology of Vibrio vulnificus and Vibrio parahaemolyticus in tropical waters. Wat. Res. 1989, 23, 923–931. [Google Scholar] [CrossRef] [Green Version]
- Boehm, A.B.; Ashbolt, N.J.; Colford, J.M.; Dunbar, L.E.; Gold, M.A.; Hansel, J.A.; Hunter, P.R.; Ichida, A.M.; McGee, C.D.; Soller, J.A.; et al. A sea change ahead for recreational water quality criteria. J. Water Health 2009, 7, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Field, K.G.; Samadpour, M. Fecal source tracking, the indicator paradigm, and managing water quality. Water Res. 2007, 41, 3517–3538. [Google Scholar] [CrossRef]
- Hardwood, V.J.; Staley, C.; Badgley, B.D.; Borges, K.; Korajkic, A. Microbial source tracking markers for detection of fecal contamination in environmental waters: Relationships between pathogens and human health outcomes. FEMS Microbiol. 2014, 38, 1–40. [Google Scholar] [CrossRef] [Green Version]
- Korajkic, A.; McMinn, B.R.; Harwood, V.J. Relationships between microbial indicators and pathogens in recreational water settings. Int. J. Env. Res. Public Health 2018, 15, 2842. [Google Scholar] [CrossRef] [Green Version]
- Paolino, G.; Vaira, F.; Mercuri, S.R.; Di Nicola, M.R. Fast recognition of Loxosceles rufescens in Italian spider bites to avoid misdiagnosis, alarmism and start a prompt treatment. J. Eur. Acad. Derm. Venereol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Moran, K.; Webber, J. Surf, sand, scrapes and stings: First aid incidents involving children at New Zealand beaches, 2007–2012. J. Paediatr. Child Health 2014, 50, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Petronis, K.A.; Welch, J.C.; Pruitt, C.W. Independent risk factors for beach-related injuries in children. Clin. Pediatrics 2009, 48, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Abdelzaher, A.M.; Wright, M.E.; Ortega, C.; Hasan, A.R.; Shibata, T.; Solo-Gabriele, H.M.; Kish, J.; Withum, K.; He, G.; Elmir, S.M.; et al. Daily Measures of Microbes and Human Health at a Non-point Source Marine Beach. J. Water Health 2011, 9, 443–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitman, R.L.; Harwood, V.J.; Edge, T.A.; Nevers, M.B.; Byappanahalli, M.; Vijayavel, K.; Brandão, J.; Sadowsky, M.J.; Wheeler Alm, E.; Crowe, A.; et al. Microbes in beach sands: Integrating environment, ecology and public health. Rev. Environ. Sci. Biotechnol. 2014, 13, 329–368. [Google Scholar] [CrossRef] [Green Version]
- Solo-Gabriele, H.M.; Harwood, V.J.; Kay, D.; Fujioka, R.S.; Sadowsky, M.J.; Whitman, R.L.; Wither, A.; Caniça, M.; Carvalho da Fonseca, R.; Duarte, A.; et al. Beach Sand and the Potential for Infectious Disease Transmission: Observations and Recommendations. J. Mar. Biol. Assoc. UK 2016, 96, 101–120. [Google Scholar] [CrossRef] [Green Version]
- Weiskerger, C.J.; Brandão, J.; Ahmed, W.; Aslan, A.; Avolio, L.; Badgley, B.D.; Boehm, A.B.; Edge, T.A.; Fleisher, J.M.; Heaney, C.D.; et al. Impacts of a changing earth on microbial dynamics and human health risks in the continuum between beach water and sand. Water Res. 2019, 162, 456–470. [Google Scholar] [CrossRef]
- Shah, A.H.; AbdelZaher, A.M.; Phillips, M.; Hernández, R.; Solo-Gabriele, H.M.; Kish, J.; Fleming, L.E. Indicator microbes correlate with pathogenic bacteria, yeasts and helminthes in sand at a subtropical recreational beach site. J. Expo. Sci. Technol. 2012, 110, 1571–1583. [Google Scholar] [CrossRef]
- Wright, M.E.; AbdelZaher, A.M.; Solo-Gabriele, H.M.; Elmir, S.; Fleming, L.E. The intertidal zone is the pathway of input of enterococci to a subtropical recreational marine beach. Water Sci. Technol. 2011, 63, 542–549. [Google Scholar] [CrossRef]
- Black, J.C.; Welday, J.N.; Buckley, B.; Ferguson, A.; Gurian, P.L.; Mena, K.D.; Yang, I.; McCandlish, E.; Solo-Gabriele, H.M. Risk assessment for children exposed to beach sands impacted by oil spill chemicals. Int. J. Environ. Res. Public Health 2016, 13, 853. [Google Scholar] [CrossRef]
- Ferguson, A.C.; Mena, K.D.; Solo-Gabriele, H.M. Assessment for oil spill chemicals: Current knowledge, data gaps and uncertainties addressing human physical health risk. Mar. Pollut. Bull. 2020, 150, 110746. [Google Scholar] [CrossRef]


| Location | Average Duration of Time Spent at This Location Per Child (Seconds) | No. of Children Who Spent Most of Their Time at This Location |
|---|---|---|
| Seawater | 1556 | 5 |
| Intertidal | 1069 | 2 |
| Dune ridge | 741 | 2 |
| Berm crest | 303 | 1 |
| Sandbar | 15.4 | 0 |
| Back beach | 6.4 | 0 |
| Dune areas | 2.8 | 0 |
| Boardwalk | 0.1 | 0 |
| Not in view | 2.9 | 0 |
| Body Part where Abrasion Occurred | Total Number of Existing Abrasions | Total Number of New Abrasions | Amount Total Abrasions (%) |
|---|---|---|---|
| Hand | 5 | 0 | 3.5% |
| Elbow | 2 | 0 | 1.4% |
| Arm | 23 | 0 | 16.0% |
| Knee | 23 | 3 | 16.0% |
| Leg | 61 | 2 | 42.4% |
| Feet | 8 | 1 | 5.6% |
| Front torso | 5 | 2 | 3.5% |
| Back | 8 | 0 | 5.6% |
| Head | 9 | 2 | 6.3% |
| Total | 144 | 10 |
| Type of Abrasion | Miami-Dade County | Galveston County | ||||
|---|---|---|---|---|---|---|
| No. of Children with Abrasions | Percentage of Children with Abrasions (%) | Confidence Interval | No. of Children with Abrasions | Percentage of Children with Abrasions (%) | Confidence Interval | |
| Non-insect only | 20 | 50.0% | 0.34 to 0.66 | 13 | 38.2% | 0.22 to 0.56 |
| Insect bites only | 9 | 22.5% | 0.11 to 0.39 | 14 | 41.2% | 0.25 to 0.59 |
| Both non-insect and insect bites | 11 | 27.5% | 0.15 to 0.44 | 7 | 20.6% | 0.087 to 0.38 |
| Total | 40 | Total | 34 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomenchok, L.E.; Gidley, M.L.; Mena, K.D.; Ferguson, A.C.; Solo-Gabriele, H.M. Children’s Abrasions in Recreational Beach Areas and a Review of Possible Wound Infections. Int. J. Environ. Res. Public Health 2020, 17, 4060. https://doi.org/10.3390/ijerph17114060
Tomenchok LE, Gidley ML, Mena KD, Ferguson AC, Solo-Gabriele HM. Children’s Abrasions in Recreational Beach Areas and a Review of Possible Wound Infections. International Journal of Environmental Research and Public Health. 2020; 17(11):4060. https://doi.org/10.3390/ijerph17114060
Chicago/Turabian StyleTomenchok, Lara E., Maribeth L. Gidley, Kristina D. Mena, Alesia C. Ferguson, and Helena M. Solo-Gabriele. 2020. "Children’s Abrasions in Recreational Beach Areas and a Review of Possible Wound Infections" International Journal of Environmental Research and Public Health 17, no. 11: 4060. https://doi.org/10.3390/ijerph17114060